Cancer strikes fear in everybody because in most cases the disease is incurable. But over the years medicine has advanced to an extent that most cancers are now manageable, and the lives of patients extended considerably.
One of the techniques developed for cancer treatments is the use of cancer genetic signature or predictor to provide the best cancer care for patients.
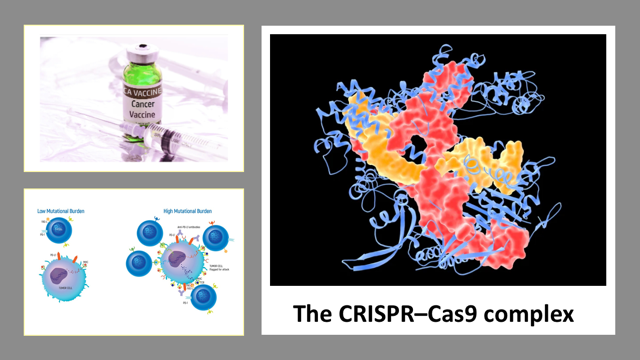
Join our WhatsApp ChannelAs part of cancer management, cancer DNA is sequenced to identify specific mutations. Tumours (or cancers) having many mutations tend to respond well to drugs known as immune checkpoint inhibitors (ICI). This class of drugs trains the body’s immune system to recognise and attack cancers.
READ ALSO: New Cancer Vaccines Raise Hope
Cancers with many mutations are said to have high tumour mutational burden (TMB). In other words, TMB measures the total number of mutations that result in a change in proteins. A change in a protein result from a cascade of changes: mutations result in changes in DNA, and changes in DNA lead to changes in amino acid. When changes occur in amino acid, the result is a change in protein. These new proteins with new shapes are called neo-antigens because your body does not recognise them, therefore, your immune system classifies them as foreign. The immune checkpoint inhibitors stimulate and allow the immune system to detect these new proteins (i.e. neo-antigens) and in the process destroy the cancer. It must be stressed that inherited mutations are in most cases not recognised as foreign by the body immune system. Therefore, such mutations are not included when calculating tumour mutational burden (TMB).
Biomarkers such as TMB are important in cancer treatment as tools used in predicting which patients are most likely to respond well to immunotherapy. Pembrolizumab (brand name, Keytruda) is an immune checkpoint inhibitor for the treatment of cancers with high TMB found in such cancers as lung, cervical, kidney, and liver cancers.
To determine the TMB of a cancer patient, the tumour DNA is sequenced, and the sequences compared against reference genomes in databases made up of sequenced data from thousands of people. But as recently reported by Nassar and coworkers in the October 2022 issue of the journal, Cancer Cell, tumours of people with European ancestries when compared with a reference panel, showed a 50% higher TMB than was true. Whereas patients of African and Asian ancestries showed TMB overestimation twice as high as their actual TMB!
To put the import of this finding into proper context, a dose of the drug, pembrolizumab, costs $10K. This means that patients with African and Asian ancestries are being prescribed an expensive drug that is useless or makes little or no impact to their condition.
The team used an algorithm to compare disease and reference genomes in the databases. Patients with European ancestry had 21% overestimation of TMB-high compared with patients of Asian ancestries who had 37%, and those of African descent who had 44% false positives of TMB-high!
When the researchers applied a corrected algorithm to patients with non-small cell lung cancer who had received immunotherapy (i.e. immune checkpoint inhibitor therapy) based on TMB-high, the result showed that only patients of European descents had significantly improved conditions. Survival rates were not improved for patients of non-European descents. Additionally, it was discovered that patients with Asian ancestries suffering from certain cancers and who received immunotherapy, were less likely to survive or have their condition improved.
The cause of this discrepancy is in part due to by poor recruitment of non-European patients during trials of such immune checkpoint inhibitor studies, in fact, less than 4% of patients with African descents are recruited to participate in such trials. To fix this problem, TMB test in patients of African and Indian descents should be done by comparing the patient’s tumour with their own normal DNA, instead of with a reference panel, since that reference panel is generated with mostly genomes of people of European descents.
Non-European patients are typically predisposed to getting low quality of care. The problem is further exacerbated by systemic racism and discrimination culminating in people of African ancestries having the highest cancer mortality rate when compared with people from other ancestries.
Meanwhile a new therapeutic cancer vaccine against advanced breast cancer has undergone a successful Phase I nonrandomised clinical trial. This was announced in the November 2022 issue of the journal, JAMA Oncology, by Disis and coworkers.
Plasmid DNA vaccine involves the delivery into the nucleus of a cell, a plasmid DNA encoding the DNA blueprint for the synthesis of the desired protein (or antigen) against which an immune response is targeted. When the cell synthesised the protein, it triggers an immune response.
About 30% of breast cancers are HER2-positives. HER2-positive breast cancer is associated with the overproduction of a protein called Human Epidermal growth factor Receptor 2 (or HER2). This protein is encoded by the gene ERBB2 (HER2 and ERBB2 are often used interchangeably). The HER2 protein promotes the growth of cancer cells, therefore, HER2-positive cancers are often more aggressive than other types of breast cancer because they grow faster and are prone to reoccurrence.
One of the effective treatments of HER2 breast cancer is the use of monoclonal antibody, which blocks the activity of the HER2 protein on cancer cells. But the new DNA vaccine being developed by Disis and coworkers, prompts cells to produce a specific fragment of the HER2 protein, which then triggers an immune response against the cancer cells. In brief, the plasmid DNA vaccine encoded the ERBB2 intracellular domain and when administered to patients, generates dose-dependent ERBB2-specific immunity.
Desis and coworkers started this study 20 years ago, enrolling 66 people of ages between 34 and 77 with advanced HER2-breast cancer (or ERBB2-breast cancer). The Phase I clinical trial was specifically designed to test the safety of the vaccine because HER2 protein is also present on other cell types in the body. Therefore, the Phase I clinical trial was a 10-year followup for each participant to observe any problems arising from antibody activity against healthy tissues. Three different dose levels were tested to evaluate the long-term safety of the vaccine.
The data generated from the clinical trial did not only show that the vaccine was very safe, but participants had better overall survival outcomes, with 80% of the participants surviving the full 10-year followup. This contrasts with the fact that only about 50% of patients with advanced HER2-breast cancer survive for more than five years.
The Phase II randomised-controlled clinical trial, which started a few years ago and nearing completion, is testing the efficacy of the vaccine by employing larger sample population. And if the result is as good as the initial Phase I clinical trial, the researchers plan to rapidly move onto Phase III. So, chances are that soon, we may be having an effective vaccine against the deadliest type of breast cancer.
In another development, a preprint article in the 10 November 2022 edition of the journal, Nature, by Foy and coworkers, indicates the possibility of the use of the CRISPR gene-editing technology to modify immune T cells so that they are better able to recognise and destroy a person’s cancer cells.
A small clinical trial involving 16 people with solid tumours, including in the breast and colon, were conducted by Foy and coworkers. The workers sequenced DNA from blood samples and tumour biopsies. The aim was to look for mutations present in the tumour but absent in the blood. They had to carry out this procedure for each of the patients. This is because cancer in a minority of cases have shared mutations but often, mutations are different in every cancer.
The workers then employed algorithms to predict which of the mutations were likely to be capable of provoking a response from T cells. Remember that T cells or T lymphocytes are a type of white blood cells derived from stem cells in bone marrows. They are part of the body’s immune systems and are adept at killing anything the body considers as foreign.
But also remember that cancer has the tendency to grow and reproduce uncontrollably so that healthy cells are invaded. Therefore, the T cells are in most cases overwhelmed by the rapid growth of cancer cells, and because cancer cells are mutated versions of the body’s own cells, the body in certain cases do not recognise them as foreign. To add to the mix, cancer cells are also capable of suppressing immune responses by releasing immune-suppressing chemical signals.
The researchers therefore, built T cell receptors that are capable of recognising cancer mutations. Using the CRISPR genome editing, the receptors were inserted into the T cells of each participant. The result showed that the edited cells circulated in the blood of recipients and were found in higher concentrations nearer cancer cells than non CRISPR-edited cells.
A month after receiving the engineered T cells, it was discovered that the cancers in 5 of the patients had stopped growing. And only 2 out of the 16 patients experienced side effects, which were ascribed to the activity of the edited T cells.
This is a proof of principle demonstrating the fact that it is possible to create an army of a person’s immune cells capable of hunting down and destroying cancer cells. And with so many concerted research efforts on cancer by scientists, the days when cancer equates to a death sentence are fast nearing an end.













![Trump, Zelenskyy Discuss Peace Plans During Pope Francis’ Funeral In Rome [VIDEO]](https://www.primebusiness.africa/wp-content/uploads/2025/04/Trump-and-Zelenksy-meet-at-Pope-Francis-Burial-150x150.jpeg)



Follow Us